 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv U.S. House of Representatives CSPAN August 26, 2009 5:00pm-8:00pm EDT
5:00 pm

we want to continue the continuity of operations in the event of any catastrophe or in the event of half of the government employees will be effected by this terrible virus. . .
5:01 pm

identifies how the department of defense community and the civilian community and the intelligence community can work together to work on procedures and controls to improve the security of our country's information systems. very, very important to gen. -- important event. we will continue our series over social media. two programmes per month. in october we will be talking about government 2.04 mobile applications -- 2.0 for mobile applications.
5:02 pm

exciting events. some very important announcements today. the potomac forum will be hosting a large event on open- source and government. open-source and government will take place in the ronald reagan building. it will consist of four tracks focusing on using that for innovation and management. for our government. keeping the initiatives from the administration. stay tuned to our website for that information. tomorrow, tomorrow was very exciting. we'll be talking about innovation. contests. crowd forcing. all the fun things -- >> this event is wrapping up with housekeeping.
5:03 pm

tonight, an in-depth look at medicare, part 8. our guest is the former administrator for medicare and medicaid. that is tonight at 8:00 p.m. eastern. >> as the debate over health care continues, our health care how does an online resource. -- our health care website is a resource, including video from town hall meetings you have gone too. and there is more at c- span.org/healthcare. >> flags are flying at half staff today. senator ted kennedy passed away last night. president obama singing this morning that the massachusetts's senator's ideas are stamped on scores of laws and reflected in
5:04 pm

millions of lives. >> sustained by remember priceless years together, i will try to carry for that special commitment to justice, excellence, a justice that distinguish their lives. [applause] >> an extraordinary opportunity for impacting events in the senate and i think this is enormously rewarding. it has had its ups and downs but i have enjoyed it and found it rewarding. >> senator ted kennedy will lie in repose at the john f. kennedy library thursday and friday and his funeral will be in a catholic church saturday and buried at arlington national
5:05 pm

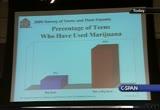
cemetery saturday afternoon. c-span will remember senator kennedy with some of his speeches and tributes starting after 9:00 tonight. >> a new survey finds teenagers who have seen their parents drug are more likely to use cigarettes, alcohol, and marijuana. this was conducted by the national center on substance abuse, a.k.a. "casa." the health and education secretary during the carter secretary -- during the carter administration speaks now. this is about half an hour.
5:06 pm

>> we are having some technical problems. we wanted to let john know about the lineup involving senator kennedy, president obama talking about senator kennedy, biden, as senator reid, and the speech from 1980 and one from 2008. that program is ready now -- a survey on teenagers who have seen their parents drug are much more likely to use alcohol, cigarettes, and marijuana.
5:07 pm

[captioning performed by national captioning institute] [captions copyright national cable satellite corp. 2009] >> good morning. i am the founder and the chair of the substance abuse program at columbia university. also with me is david rosenblum, casa's president and chief executive officer. this morning we are releasing the 14th national survey of american attitudes on substance abuse. this year's back-to-school survey continues our unique effort to identify and track attitudes of teenagers and those parents who influenced them.
5:08 pm

over one decade and a half through the survey, we have identified factors that increase or decrease the likelihood of a teenage substance abuse. armed with this knowledge we believe parents, teachers, and coaches have been better able to help us grow up drug trade. we regard this as a work in progress as we try each year to improve our ability to improve the situation said and characteristics that influence the risks that a teenager will smoke, drink, use illegal drugs, or abuse prescription drugs. . a number of government surveys conducted epidemiological surveys.
5:09 pm

this survey asks questions such as how many of the teenagers's friends smoke or do drugs, or what percentage of the parties the teenager bataan's -- the teenager it tends to -- the teenager attends is alcohol used. we have identified a number of circumstances and characteristics. they affect the teenager's risk of smoking, drinking, and using drugs. we have learned how stress, boredom, spending money, parties, hanging out on school nights, eating disorders, conduct disorders, and transitions like puberty and changing schools affected teenager's risk of smoking or using drugs or drinking.
5:10 pm

for drug years, if you want to buy marijuana now, how fast could you get at? we have gained insight into america's teenage culture. perhaps our most important findings are these -- a child who gets to age 21 without smoking, without using illegal drugs, and without abusing alcohol is virtually certain never to do so. the greatest influence on children? parents. no one has greater power to influence a teenager's decision whether to smoke, drink, or use drugs than that teenager's mother or father. this survey sends an alarm to parents, to parents of teenagers who drink. mom and dad, if you're a teenager drinks, the odds are your teenager is getting drunk.
5:11 pm

two-thirds of teenagers who drank at least once per month get drunk at least once per month. to put that into perspective, the risk behavior survey of 2007 of the center for disease control and prediction -- and prevention found 44.7% of high- school students had one drink within the last month. this year's survey identifies some parents who have become enablers of their teenager's smoking and drug use. by their attitudes and conduct they send their 12-year-old to 17-year-olds the message that is ok to smoke, drink, and use drugs like marijuana. parents who get drunk in front of their children are enablers. fathers who are ok with their
5:12 pm

12-year-old or 17-year-olds drinking are enablers tensor mothers and fathers who expect their children to use drugs and to acquiesce in sending their children to schools where the drugs are used, capped, and sold. team -- teen behavior is associated with parental expectations and behavior. parents who expect their parents -- to have children who smoke can use drugs will have children who smoke and use drugs. it is a mom-and-pop operation. my new book, "how to raise eight drug-free kits," which was published earlier this month -- "how to raise a drug-free kid" offers evidence-based advised on
5:13 pm

how to be engaged with their children, talking to kids about the dangers of tobacco, alcohol, and drug use, and having high expectations and setting and enforcing limits and providing a good example. although written by me, this product is the product of two decades of work by scores of professional researchers. it is published as an original paperback so that any parent can afford this and all royalties go andcasa -- to go -- go to casa to combat substance abuse. the bottom line is this -- do not be vague about expectations. let them know clearly and consistently that you do not approve of underage drinking. set high expectations for your children and for your school
5:14 pm

environment. show them through your own engagement, your own behavior, how you live by those expectations. remember,. pressure trump's peer pressure. -- remember that parental pressures trumps peer pressure. for the past years, she has managed our annual survey and she has been assisted by roger vorn and associate editor for statistics and evaluation steve wagner. as well as a distinguished outside advisory group. it is elizabeth's standards and creativity, to say nothing of the fact that she is the mother of three children, that is primarily responsible for this
5:15 pm

undertaking. she will now report the survey findings and take your questions. >> i am going to walk you through the findings for our 14th national survey of american attitudes on substance abuse. over the years that we have conducted this survey, we have noted attitudes and behaviors that make teenage substance use more or less likely. this year's survey shows how words and expectations are related to their kids behavior's and the findings remind us that for better or worse, parents have a tremendous impact on whether or not their kids will use substances. i will take you through the key findings and highlight some of the most important points. i want to take a moment to
5:16 pm

acknowledge our survey advisers. this group of advisers are independent advisers and research experts and they have been helping us for a number of years. they reviewed the analysis and the presentation on the findings and they help us with the survey methodology every year. in the folders you have received you have complete copies of the report. you have copies of the questionnaires. the teenage questionnaire and apparent questionnaire and you have a lengthy description of the survey methodology. i hope you take a look at it and if you have questions, we are available to address this. this is just a snapshot of the methodology. we conduct the survey every spring. before the survey, in the winter we conduct focus groups and we use the focus groups -- those of us who work on the survey are
5:17 pm

distant from our teenage years so we use the group said that when we send down with the teenagers they can inform us about what is going on today in teenage culture. they help us in developing new questions for the survey and they help us make sure when we are crafting the questions that the kids are hearing the question as we mean that when we ask the question. we do that in the winter. this past winter we had two focus groups -- high school juniors and seniors that we met with and we also met with a group of recent high-school graduates. we ask them to reflect back on their high school experience. in the spring we went out with our survey. this is drawn from a nationally representative cycle. the teenagers are randomly selected. this year we completed 509 interviews with boys between the ages of 12 and 17 and 491 interviews with girls between 12
5:18 pm

and 17. before we speak with the teenagers, we obtain consent from their parents to speak with us. we were able to complete 452 interviews with parents. these are parents of the same teenagers that we interviewed. but we are able to do is linked the responses in a household between the teenager and the parent. what i am going to start about talking about is the theme of teenage drinking and drunkenness. we had a number of important findings this year. i am going to summarize these now. the most significant finding from this year's survey is that teenagers are getting drunk -- if they are drinking on a monthly basis they are also getting drunk on a monthly basis. this chart demonstrates that. if you look at the blue bar, 2/3 of teenagers who drink once a month also get drunk at least once a month.
5:19 pm
by the time they are 17, 85% of 17-year-olds also get drunk at least once a month. we asked teenagers if this is their intention. do they drink with the intention of getting drunk? one-third drink to get drunk. what is interesting is about this is 85% due in fact get drunk on a monthly basis when that is what they set out to do. what is also important for parents to understand is that kids answered no. they do not drink with the intention to get drug trade one- third of them get drunk on a monthly basis -- to get drunk, one-third get drunk. the relationship between teenage
5:20 pm
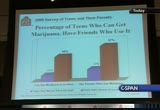
drinking and risky sexual behavior -- we know that earlier they drink the more likely they are to have drinking problems later in life. what we looked at is the relationship between teenage drunkenness and other substance use. as you can see in this chart, compared to teenagers who have never tried alcohol. those who have gotten drunk are 18 times likelier to have tried marijuana. this may be because of the crowd that they are moving denture. teen-agers who get drunk on a monthly basis are four times likelier to say that they can get their hands on marijuana in one hour. there are three times likelier to have friends who are using this drug. you see the relationship between teenage drunk in nests and friends who use other substances. teen-agers who get drunk monthly are three times likely to have friends who are misusing
5:21 pm
prescription drugs and 2.5 times like here -- black clear to have friends who use drugs such as ecstasy, math, or lsd -- meth, or lsd. parents are incredibly important in influencing teenage attitudes and their behavior. we have findings about how important mothers are in kids' lives and we decided to take a look at dad. i want to make sure that dads are on the hope, too. what we asked teenagers, the question that drove this series is, how do think your father feels about you drinking? ok with it or against it? when teenagers think that their parents are ok with them drinking, they are 2.5 times likelier to get drunk in a month. that is very important.
5:22 pm

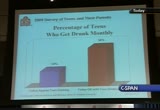
i can tell you that this perception that your dad is ok with you drinking is ok among the oldest boys in our survey. 20% of the boys that we surveyed thought that their dad is ok with them drinking. how do you think that parents feel about you drinking as an important element, an important factor in the kids' attitudes and behavior, but also the behavior that the parents model for you is important. what they say is important but what they do is important as well. we asked if they have seen their parents get drunk. one-third of the 12 year-olds to 17-year-olds have seen their parents strong. by the age of 17, half of the 17-year-olds have seen their parents drunk. this is how seeing their parents
5:23 pm
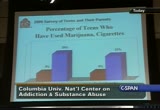
drug relates to their behavior. compared to teenagers who have never seen their parents strunt , their 2.5 times likelier to drink alcohol and likelier to drink on a monthly basis. mimicking the activity -- teenagers who have seen their parents drunk are 2.5 times likelier to get drunk on a monthly basis. seeing your parents' drug is also related to other substance abuse. -- drunk is also related to substance abuse. three times likely to try cigarettes. what we are interested in this year was how teenage added to its impact their behavior. this is driven by a new question this year. we ask, do you think that the decision to use marijuana by someone your age is a big deal?
5:24 pm
is it an important or serious question, or not a big deal? the youngest kids only 10% said not a big deal. by the time they are 17 percent -- by the time they're 1740% say it is not a big deal. how they feel about this decision is directly related to their behavior. compared to the kids who think that it would be a big deal to use marijuana, those who think it is not such a big deal are four times likelier to try this drug. interestingly, when teenagers have tried cigarettes, over half of them say the decision to use marijuana is not a big deal. in 2004, we released in conjunction with the american legacy foundation we released a report on cigarettes and
5:25 pm

marijuana use and we looked at how cigarettes impacted their behavior with respect to marijuana. what we see here is a follow-up -- how cigarette impacts their attitudes with respect to marijuana. these are other aspects that are related to their attitudes about pot use. large majorities of teenagers to get good grades in school and have an excellent relationship with their parents and to attend religious services weekly say that the decision to use marijuana is a big deal. so we have looked at how teenage attitudes affect their behavior with respect to marijuana. we are interested in their parents' attitudes about the drug. this is a snapshot on how the parents stand. almost all of them -- 96% say it is important to them that they're teenagers not use
5:26 pm
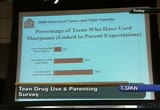
marijuana. 93% believe that the drug is harmful to some one of the age of their children but for report% say it is unrealistic to expect that the teenager will not use this drug. here we see how parent expectations went with their kids' behavior. we are linking the parent expenses and the child responses within households. -- parent responses and child responses within households. how likely do you think that your child will use drugs in the future? never? not likely? very likely? we linked this to the children's responses. teenagers whose parents think that future drug use is likely are 10 times likelier to use
5:27 pm
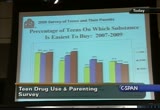
marijuana than that teenagers whose parents say that the future drug use will never happen. we have looked at attitudes and behavior and now we're going to look at the availability of marijuana and prescription drugs to teenagers particularly with respect to prescription drugs. we have new findings. this is a question we have been looking at for years. we ask, what substance is easiest to buy -- cigarettes, marijuana, prescription drugs for the purpose of getting high, or beer? marijuana is as easy to buy as cigarettes. since 2007, 37% increase in the percentage of kids who say that marijuana is the easiest to buy and prescription drugs are third on the list. a question that we use -- joe references this in his remarks -- a question to get a sense of
5:28 pm
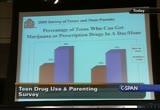
the proximity of drugs in kids' lives as we ask them if you wanted to get marijuana right now, how long would it take you to get? if you look at the marijuana bars, 23% say that it would only take them one hour to get their hands on marijuana and 40% would be able to get the drug in one day. this chart does not tell you the trend but i can tie you we have been looking at these trends for years and they are virtually identical. for the first time this year we asked the same question with respect to prescription drugs. if you wanted to get prescription drugs right now for the purpose of getting high, how long would it take you to get them? almost one in five can get it in just wonder one hour. a little over one-third within one day. if we applied these percentages
5:29 pm
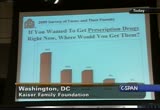
, almost 9 million can get them within one day. where do we get them? if you want to get prescription drugs right now, where would you get them? one-third would be unable to get them, but what we show you are the next most popular response options. most kids to say that they can get prescription drugs are getting them from home, their parents, family members, or their friends. this is what it looks like for marijuana -- if you wanted to get marijuana right now, where would you get this? one-quarter of them would go to their friends. 13% say that they would get their drugs from school. presumably from other students, but we do not know.
5:30 pm
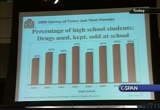
drugs in school is a topic that casa has been tracking for many years. we ask kids every year, is your school drug-free or is it not drug-free? meeting some kids keep, use, or sell drugs after school? two-thirds of the high school students that we surveyed said that drugs are used, kept, or sold at their school. this has been pretty consistently the case for the past five years. this is what the middle school students said about one-quarter of them say that drugs are used, kept, sold at school. we see a little bit in the decline since 2007. why do we care about drugs in schools? when drugs are available on the grounds drugs are much more --
5:31 pm
the kids are much likelier to get them quickly. when we look at kids responses and their responses to how quickly they could get substances, kids to say that drugs are present at their school three times likelier to be able to get their hands on marijuana in one hour and they are twice as likely to get prescription drugs for the purpose of getting high in just one hour. to many parents except the facts of drugs in our schools. 89% of the parents surveyed said it is important that their kid'' school is drug-free, but 60% say that their child's school is not a drug-free. drugs are used, a cat, or sold on the grounds of the school. when i showed you earlier than
5:32 pm

non-drug-free schools, when we look at all of the teenagers, 45% say that their school is not drug-free, but more believe that the schools are not drug-free. the parents may have a more realistic view. what is interesting is that among these parents who say that drugs are present at their school, 62% eight is more likely that they're teenagers will use drugs if there are drugs on the school grounds and they are right. we have research that shows the connection between the presence of the drugs at school and the likelihood that the teenagers who go to do schools will use those drugs. more than half say that the goal of a drug-free school is not realistic and 45% say there's nothing parents can do and only one-quarter of these parents have never talk to anyone -- a teacher or administrator -- about this problem. parents do not think there is anything they can do to achieve
5:33 pm

a drug-free school and their interaction may help to ensure that schools continue to be places where kids keep, use, and sell drugs. to help affect change, we have devoted a chapter in their book on how to raise eight drug-free kid on educating parents about drugs in schools and describing how they can raise the issue with administrators of this school. the book is packed with practical advice about talking to your kids about drug use and answering their questions about what you did when you were a teenager and understand the difference between boys and girls and preparing our kids for college. casa has spent years finding out which factors make kids more or less likely to use, and which parenting actions are most effective. everything we know today about
5:34 pm

practical parenting tips is contained in the book and we invite you to visit the web site, which you can see here, straightdopeforparents.org. questions? i am happy to take them out. please wait for the microphone. >> to break down -- milliken, with the am media -- to break down the questioning further, i am just glancing through the survey questions, are you able to find out -- i see you have a question on religious preferences. do you make any distinctions among the various religions on how that affects the alcohol and drug abuse? also, on the frequency of worshiper-relations attendance
5:35 pm

-- worshiper-religious attendance, how that may affect that. when it comes to alcohol, do you make any distinctions as far as the type of of all? beer, wine, harter -- harder, larger amounts of bohol? >> let me take the religious question. we have seen a trend over a number of gears that kids who attend religious services on a weekly basis are much less likely to be using substances compared to their peers who do not attend religious services. we have done a lot of research on spiritual practice and spirituality and substance abuse risk. in the case of teenagers, when kids are going to religious services, they go with their parents. that relates to parental engagement. that is something we have looked
5:36 pm

at over the years. in terms of the alcohol, what is the alcohol they are drinking? teen-agers tend to prefer the taste of liquor mixed with something sweet. in terms of this year's survey and the statistics on drinking and drunken s, we did not ask them to distinguish what they were drinking. i do not think we have ever seen -- >> [inaudible] >> we do not have a large enough sample of the other. >> differences? >> between christian and non- -- no, there is no breakdown. >> when you talk about mixing drinks, you said that was last year's survey?
5:37 pm

did you find -- what was the alcohol of choice? >> we do not know. ok. thank you so much. ñ >> tonight, an in-depth look at medicare part a, dealing with
5:38 pm

hospital insurance. our guest is the former administrator for medicare and medicaid in the bush administration. tonight at 8:00 p.m. eastern. special middle east on boy george mitchell released a statement today praising progress on the peace progress. more about that now with the state department spokesman ian kellee. he begins with a statement on the death of ted kennedy. this is a half-hour. >> ok. good afternoon. welcome again to the state department on this fine august day. i would like to recognize the professor of my almaguer -- the president of my armor -- my alma mater. unfindable large college. i highly recommend it if anyone is looking for it. -- a fine college.
5:39 pm

i highly recommend it. senator kennedy -- you will note that she said that his legacy will live on in the hearts and minds of millions of americans who are freer, healthier, and more prosperous because of his efforts. the work goes on, the cause indoors, the hopes still lives, and a dream shall never die. we have statements from special envoy mitchell, who knew senator kennedy very well. in addition, a statement from our ambassador to india that we're also going to forward. but those brief remarks, i will take questions. >> can you elaborate at all on the very productive and good
5:40 pm

progress, what it means? >> as they noted in their statement, we plan to continue talks next week. there will be a delegation coming from israel to talk to a special envoy michel. -- mitchell. we do want to make sure that these talks continue to have forward movement, as you noted. that they make good progress. i did not note that. the statement noted that. >> the statement noted that. let's let these talks play out. we have another set next week. there is room for optimism. i do not want to get into anything that will in any way cause any kind of obstruction to
5:41 pm

this movement. dave? >> in connection with the guardian newspaper, the story on the breakthrough in the middle east, one of the tenants of the store was that the united states is prepared to link its policy with iran. in other words, a harder line on iran by the united states. an incentive for the israelis. can you comment? >> this is very important to this administration, the idea of comprehensive peace. this is an important objective. because these are sensitive and critical investigations, i really do not want to comment on any of these. we do not want to suggest that there is any necessarily break through, there.
5:42 pm

we have an ongoing process and we want to give that a chance to work. >> i would like to go back to the statement. where is the secretary today? >> the secretary is out of the office. >> where is she? exactly? >> her particular vacation plans are not something -- it is not a news story. >> is she going to attend the ceremony? >> i do not now. the services? i do not know. not me see if i can find that out. >i do not know. >> he said the parties had agreed on meaningful negotiations. what do you mean? >> everything that we are doing
5:43 pm

now is to lay the foundation for the negotiations. for israel and palestinian representatives to sit down and come to a negotiated solution. >> who would the israeli delegation -- >> i do not know. if you call the israeli embassy they will tell you. it is up to them. >> to you know when next week? >> i do not have the dates. i believe it is in washington. >> the statement said the united states -- >> the united states. >> netanyahu said that he was making headway in diffusing the resettlement.
5:44 pm

he said he wants a compromise to proceed with some settlement. is the u.s. prepared to agree to that? >> i do not think you will be surprised by my answer. we want to keep these negotiations in a confidential, diplomatic track. i am not going to try to characterize what the prime minister said and i am not going to try to characterize -- >> the other day you were very clear about saying no concessions. has that changed? >> i beg your forbearance. it is a sensitive time. i do not want to get into that. >> you are suggesting that she made -- >> i am not suggesting anything. i am not going to comment.
5:45 pm

quite she is right. the other day. you said all settlements must not. all means all. >> that has been our position. >> no longer? >> i am going to let mitcvhe -- mitchell negotiate. >> so this is a negotiable position? >> i am not saying that. i am not retracting my words. in this not appropriate for me to put myself in this process. again -- same answer. i am not going to try and characterize exactly what happened in the meeting. >> the other thing that came out of this is that both sides indicated that the israeli and palestinian leaders had their
5:46 pm

first meeting in the coming weeks. is that your understanding? >> broken record. i am not going to characterize our standing of these confidential negotiations. >> a final settlement in the middle east? >> i hope so. i hope it is very soon. >> carter talked about the expectation in the coming days, some kind of comprehensive peace goals. could you clarify that for us? is that your expectation as well? >> i have gutsiness, i am not aware. -- i have not seen his comments. i am not aware of that.
5:47 pm

i am not aware of any plans like that. we will come back to you. >> the ambassador has said there will be a meeting between president obama and abbas next month. >> would not be surprised. you have to ask the white house. >> five days before the 70th anniversary of the outbreak of the second world war, washington has not yet announced whether it would recognize government in poland that which is going to be a huge event attended by chancellor merkel, putin, other
5:48 pm

heads of state. could you tell us who's going to poland from the u.s. government? why haven't you announced it before? >> first of all, let me say i think we all recognize what an important date this is. the 70th anniversary of the start of world war ii. i think everybody in europe recognizes the extraordinary sacrifices that the polish people make. we, of course, will send an appropriately senior person to this event. i know that the white house is
5:49 pm

going to make an announcement on a delegation. it is not something that will necessarily come out of the state department. >> clinton is not going? >> i am not aware that she's going to poland. it is for the white house to decide who leaves and who will be in the delegation. >> in afghanistan -- what the nato forces are doing. >> first of all, as we have said many times, this is a high priority for this administration to help afghanistan and helped in its democratic process and its
5:50 pm

rebuilding and help it become an economically viable and prosperous society. the state department has a role in that as a u.s. agency for international development. the issue of protection i think is primarily an issue for the department of defense. for details on these kinds of protection issues, you probably should address this to -- >> for many years now. do you think under the new government of afghanistan this will change? >> of course, we want to try and enable the afghan government to take responsibility not only for reconstruction but security. we have programs in place to
5:51 pm

help train them to be able to take on a lot of these responsibilities. that said, many times we are in the middle of an electoral process. we want to remain in personal regarding the candidates. you know the incumbent president is one of the candidates. >> many iranians are on hunger strikes and they will continue until they get their human rights and the rule of law. they are seeking justice. freedom. >> week -- we are watching very closely what is happening in iran.
5:52 pm

we have said consistently that the regime in iran has to respect the will of the iranian people and respect their fundamental human rights. i think you know that one of the detainees on trial right now in the revolutionary court is an american citizen. he has not been given a lawyer. we believe the charges that he is facing are without foundation. we have consistently called for his release. he poses absolutely no threat to the iranian government or its
5:53 pm

national security. he played absolutely no role in the election. he is a scholar. he is devoted his life to promoting understanding between the iranian people and the american people. he has scrupulously state politically neutral. i will close by saying that the world is watching what is going on in iran right now. we will bear witness to what is going on. >> as far as the hundred strikers are concerned, the secretary is going to do something? meet with them? >> i am just finding out from you that there are hundred strikers in front of the white house. let me see if i can find out some more information. >> family is divided by the
5:54 pm

border can begin meeting again. more than 100,000 u.s. citizens who have family in north korea -- do we have planned to meet north korea and discussed the family issue separate from the nuclear issue? >> first of all, let me say that we encourage and support efforts that are aimed at family reunification? these are important and emotional issues. these kinds of contact between north korea and south korea. we encourage dialogue between the two. between north korea months of current -- and south korea. you know our policy about bilateral talks regarding the
5:55 pm

nuclear issue. this dialogue between north korea and south korea -- we encourage this. see the republic of korea for more information. >> yesterday the subject was brought up of the indictment -- >> the policy on bilateral contact with the north koreans, you said you know what it is? what is it again? can you remind us? >> it is important when you were talking about our main goal when it comes to correa -- korea, it is important that we do this in a multilateral context.
5:56 pm

there's stakeholders in the region. the context has been the six- party talks. we do not want to be disconnected from our regional partners. when we have talks with the north koreans on these kinds of security issues, we want to have these talks with our partners. >> basically, the position is the bilateral talks outside of the six party contacts would except the two of your closest asian allies? >> we do not want to disenfranchised. we want a regional solution. >> about the indictment -- you said you had not heard about that. their reaction? he was a key fun riser -- >> i do not know about that.
5:57 pm

>> there was a bomb blast. 40 killed. do you have any comment? >> we deplore these actions of violence. we know that there was a great loss of life in the bombings. our sympathies go out to the victims' families. we do not think that afghanistan will be deterred from the path that is on developing into a democratic society and prosperous economy. i do not believe that there are any american citizens involved. >> yesterday i asked you about the tensions between syria and
5:58 pm

iraq. you told me you would try to -- >> yes. hold on one second. we understand that there has been neutral recall of the ambassadors. we consider that an internal -- and internal recall of the ambassadors and consider that an internal matter. diplomatic dialogue is the best means to address the concerns of both parties. we are working with the iraqis to determine who perpetrated these horrible acts of violence. as i said, it is an internal matter for both the iraqi
5:59 pm

government and syrian government. we encourage them -- we hope this does not hinder dialogue in the countries. >> the iraqis are accusing the u.s. of being behind a latest violence in the u.s. do you think it is possible? >> we are very concerned about these reports. we are working with the iraqi government to find out exactly who is behind them. we do not have any firm information. >> you have suspicions? >> everybody has suspicions. >> is there any progress on the house-hunting front? >> how far into the briefing are week when this was raised? i do not have much of an update.
6:00 pm

we have gone over this, of course. in the exhaust this -- in exhaustive detail. we continue to redress the sensitivities involved in this visit particularly in light of his release. .
6:01 pm

we need to do this in no way that respects everyone. >> and whether cent -- senator lawton birch request to limit movements -- to limit his amendments to the u.n. headquarters district, had ever been imposed on anyone else before?
6:02 pm

>> there is something called a foreign mission act. we are still digging a bit, but under that act, we have the right to restrict travel within a certain district of u.n. headquarters. libya is not subject to that, as you know. only its diplomats. as far as i know, that is the only restriction. >> confining someone to that area, that has never been done before. >> as far as i know, that has never been done before. but there is another part of the foreign missions act, that i
6:03 pm

think have been referenced. we can impose restrictions on the use of diplomats residents. that is a very broad provision. we are hoping that -- and we are expecting that we can come to some sort of agreement where all the sensitivities can be met. related to that. >> the mayor and others say that there is an agreement only for use by the ambassadors to the un and not anyone else, not the members of the mission. >> as i say, there are provisions for that. >> that is your understanding? >> i will have to take that question. >> and iranian diplomats are subject to this radius of 25 miles? >> yes. >> what other countries are
6:04 pm

subject to this? >> i will have to take that question. >> i asked because the north korean diplomats to recently went out into special permission to leave the area. the less i think it's fair to say that north korea is also appeared >> but it is no longer a state sponsor of terrorism, nor is libya. it is my and standing that that is the -- that is not it? >> that is not yet. and maybe one but it does not the only. >> then let live -- bell libyan diplomats can currently go where they want? >> i believe that that is the case. >> you're expecting that we can come to some kind of what? >> some kind of understanding
6:05 pm

regarding where mr. cut out the -- i think -- where mr. gaddafi will stay. go ahead, charlie. >> is the united states participating in the upcoming celebrations of the 40th anniversary of his role? >> i do not think we have made any decisions on that just yet. >> a couple of things concerning the u.n. security council meeting. as the u.s. made any decision on what kind of out meeting -- outcome it wants? and what kind of feedback have you gotten from other leaders as to whether they will attend? >> those are very broad questions and i will have to say if we can give you information on that. i am not prepared right now to say. in the back. >> [unintelligible]
6:06 pm

>> let me just say, in general, we are expecting to complete our policy review. i am not going to put a time limit on it. i think that is something we are going to be looking at. before we actually conclude that review, i am not going to prejudge how it will come out. i know that secretary clinton looks forward to talking to senator webb, talking about his visits, but i am not sure when that will happen. we look forward to hearing his views in person and we respect the views in the "new york times" today. >> are you aware of the u.s.
6:07 pm

citizens arrested in sri lanka? >> i am not aware of that. thank you very much. >> tonight, an in-depth look at medicare part a dealing with hospital insurance. our guest is tom scully, a former administrator for medicare services in the george w. bush in ministration. that is tonight at 8:00 p.m. eastern, hear on c-span. -- here on c-span. tonight on booktv, reporters from the boston globe look back on the life of ted kennedy. the event was taped earlier this year and you can see it tonight at 8:00 p.m. eastern on c-span2.
6:08 pm

>> as the debate over health care continues, c-span is health care hub is a key resource. watch the latest advance, including town hall meetings and share your thoughts on the issue with your own psittacine video, including video from any town halls you get onto. and there is more at c-span.org. >> how is c-span funded? >> private donation. >> taxes. the oilers and grants and stuff like that. >> public donations. >> i do not know where the money comes from. >> contributions from donors. >> how is c-span funded? america's cable companies created c-span as a public- service. a private business initiative -- no government mandate, no government money. >> last week, alaska senate early some rakowski -- lisa
6:09 pm

murkowski held a town he -- a town hall meeting on health care issues. this is about two hours. >> >> i can only represent you well in washington d.c. when i feel i know well what if he is that you are looking for, what you are seeking. this town hall meeting, as we discuss health care reform and health care issues and insurance, it is important for you to be here but much more important for me to be here to listen to you. as much as i would love to stand here and spend the next two hours of -- telling you about
6:10 pm

everything that is in the help committee bill or not an house bill, we can do that at another time. i would like tonight to hear your comments. i am going have to put a leash on myself, because i have a tendency to want to tell you everything that is in it. and then i would not be hearing as much from you. dennis has given you the ground rules in terms of how much time we would like you to spend in terms of your comments and questions. i am going to tried exercise a little restrained here but give you the information that i believe that you are seeking. i want to thank you not only for your presence here tonight but for the comments that i have received from alaskans all over the state, these past few months. i have probably received over 5000 e-mails, handwritten letters, phone calls, and so
6:11 pm

many of you have expressed a great deal of concern with rushing health care reform through congress. at one point in time, the president said that i do not want -- of what have a bill to sign before the 15th of october. he said that line there. i heard from many of you who are very concerned about the massive spending by our federal government. it is putting debt on our children and on our grandchildren's in generations, future generations at risk of trillions of dollars in federal debt. many of you may not have an opinion on government plans, but you are concerned about the cost of your premiums, seeing double digit increases every year, and want to know what this bill is going to do to reduce that. how was this going to help me? how might going to be able to
6:12 pm

keep the insurance that i have? i have heard from many who support the actions already taken by congress, and that the president is supporting. so wherever you are coming from tonight, i really want to hear to from you. even those of you who may say that lisa is coming at this from a different perspective. i need to hear that boys, but we need to be respectful about how we deliver those opinions. i hope that everyone has received a copy of the materials that were presented to you, a packet of information that i want to take just a minute with you tonight, before we go to your questions, because i think these will provide you with all little bit of background in terms of where i am coming from and how i have formed my position on some of these issues. the first picture there, the first graph shows the exponential growth that we face
6:13 pm

in health-care costs. the president has stated it, i think every member of congress has stated it, the growth curve is not sustainable when you talk about our health care costs. osts. part of the reason for this is many people are living longer. our technology allows for that, but also we recognize that much of this is unnecessary costs. we got duplication of tests, the practice of defensive medicine, and we have certainly here in california alaska's primary care a day results in greater utilization of specialty care. to understand why our premiums are rising so much, we need to look at how we're spending money on health care. we have gone from $250 billion in the early 1970's, to over $2 trillion in mid-2000's.
6:14 pm

i will repeat, we are on an unsustainable path and a half to be addressed in what better health care reform legislation we pursue. the second graph on the bottom of the first page is the medicare cost growth projections. includes the story macaque -- medicare costs back to 1985 that shows -- cbo is the congressional budget office, a nonpartisan budget office -- this is how much they predict medicare cost will grow without any policy changes over the next 50 years of. look at that, the increase is astronomical. but the current line indicates the net balance of the medicare trust fund. in 2018, that trust fund balance goes to $0. we have a system with medice@@
6:15 pm

this is the federal spending list. i have travelled across the state and as i talked to people about what is going on with health -- -- with health care, i find that it is i don't like what you have in health care or write to like it, it is a great deal of emotion about where our federal government is going. what are you guys in washington, d.c. doing anyway? and when you put it in the context in terms of our federal spending and the national debt, you look at it and it is unprecedented what we have seen in the past, basically, 19 months when we spent $3 trillion. trillion. how can you possibly spend that? when you think about the first mls in february, just in january of the seven and $87 billion.
6:16 pm

we bailed out fannie and freddie and aig. we have that part fun at $700 billion. -- we have that tarp fund at $700 billion. we have the cash for clunkers program. and now health care proposals that could be in excess of $1 trillion. on top of everything else? tell me that you are going to do it right. tell me that you know is going to work. and by the way, we are dealing with climate change legislation. we do not know how much that is going to cost. i put these in as one of the slides to put into context what we are dealing with in terms of federal spending. our budget deficit is predicted to be close to $1.80 trillion at the end of this fiscal year.
6:17 pm

it is substantial. it is out of control. cbo, on the bottom half of the page here, is the neutral government scorekeeper. this is who we rely on in congress to assess, to analyze the legislation that we have in front of us in terms of what it would cost. they made the comments that you have before us about health care bills before the congress. i will not read them. i want you to do it because i want to get through these slides. the next one is speaking to the needs and why we are talking so much about increasing access to health care. to better understand how we're talking about -- new we're talking about when we define the number of uninsured. we have identified 47 million people that are uninsured in
6:18 pm

this country. if you look at the pie chart, if you will see that in fact some categories of those who earn more than $75,000, 19%, but choose not to purchase health care. you have those eligible for government programs such as s- chip and medicaid that are not enrolled, and those eligible for employer-sponsored plans but have not chosen. those that are without all affordable insurance options, that is around $13 million. that helps to put that into perspective. you then have some comments from the institute of social and economic research here in anchorage, which speaks to some of the issues that we face here in the state of alaska when it comes to access for those who are medicare beneficiaries. we have got a situation here in
6:19 pm

anchorage, the largest city in this state, where you have only 13 out of 75 doctors who will see new medicare beneficiaries. this is an issue that -- without discussion, it comes to mean more often than anyone else. they tell me, my mother cannot get in to see a doctor. i do not know where to go. i brought my parents up from outside. i cannot get a doctor for them. at the health care meeting we had an affair banks last week, i had a woman stand up and -- in fairbanks last week, a woman stood up and said her mother as a great doctor, but this woman is talking about moving down to anchorage, and her doctor in fairbanks said, don't do it. you will not be able to get doctor to see your mother. this is a huge, huge problem for us when we talk about access. the next light on the back
6:20 pm

there -- slide on the back there it talks about medicaid and medicaid costs. the projection from the government says that here in the state of alaska, we spend a billion dollars on the medicaid currently. under this proposal, if we pass that version, medicaid would be expanded. the cost to the state would be somewhere between $90 million every year and $130 million every year, depending on how much the federal expansion would be. this would be a cost that is passed straight onto the state. there have been discussions -- on the federal and, we would pick it up -- but ultimately it comes back to the state and is a state expense. it is something that we need to keep in context.
6:21 pm

the last slide are some thoughts about how i believe we can advance health care reform. we must have a system that guarantees insurance coverage to those with pre-existing conditions, whether diabetes or heart disease or mental illness or very generic conditions. we must deal with this. we must keep insurance companies from denying claims or canceling coverage because of newly detected condition. those who like their health insurance must be able to keep it. we have to guarantee that help decisions that are made by you and your doctor are made by you and your doctor, and not the insurance and not the federal government. we need to make sure that we are equitably reimbursing our providers for the care they provide you and your family. we need to prohibit financing
6:22 pm

health care reform on the backs of our small businesses. here in alaska, we have many small businesses. imposing an employer mandate, in my opinion, it is very difficult for us to impose this on our small businesses. we must keep them from pacing -- placing caps on how much they would treat. and we must focus on the prevention and wellness aspect, those that would reward and facilitate healthy behavior and lifestyle changes. we would create a program that would shift millions of americans from private to public coverage and eliminate the private insurance system as we know it. the president has stated that the status quo in health care is unsustainable, and i think if you look at the first page of your handout, you will agree with that. but we must recognize that building health care reform on the backs of a broken medicare
6:23 pm

system is also unacceptable. we need that structural reform that moves us away from the first services -- fee-for services. we have a great will -- a great deal of work to do in washington, it is absolutely necessary and an imperative for your congress to address health care reform that gives us a system that we are proud of, but that also gives us a government that is affordable. with that, i would like to open it up for questions. i think that dennis has laid out the ground rules. we have microphones and he will be calling on you so i am not playing favorites with anybody. but thank you for your attention for right now. [applause]
6:24 pm

>> two more comments. when we ask someone to speak and they don't get everything they want to have said said, all of you should have picked up one of these cards at the front. please give us your comments on the cards. those of you that choose not to speak publicly, please give us your comments were visit the center on the internet and e- mail her. the one other housekeeping item, this particular brochure that the senator was going through is the only one sanctioned by senator murkowski. other materials were passed out which was fine but those were not her materials. those were of different groups. nike. yes, ma'am? just stand up. as soon as i sit down, your time starts. and please tell us your name and
6:25 pm

in the time starts. >> my name is joanne. my question is, if you talk about the bureaucrats that are going to be making the decisions, how are they going to be chosen? are they going to be chosen by i s, the people? are they going to be chosen by the president? are they going to be chosen by congress? are they going to be representative of all the 50 states? are they going to part of each ethnic group? how was this going happened and at that desk? what say are we going have? >> an excellent question, one that anyone who cares about their health care for themselves or their families should be asking. i will speak to what we have laid out in the senate bill. and when i speak about the senate bill, one caveat.
6:26 pm

there is a bill that mr. the senate health education labor and pension committee, the committee i sit down. it passed out about a month ago. there is another senate version that is being crafted or worked on within the senate finance committee by a few core individuals. there is nothing of detail yet. the house has its own version of health care reform legislation. but let me just be to the senate version, because i spent about 60 hours with members of the committee going through that proposed legislation. he would basically have, for lack of a better term, a medical board that would be composed of individuals that would be selected by the secretary of health and social services. i do not believe that the
6:27 pm

president has any oversight over the selection, who might be on the medical panel. it is through the secretary. there is a great deal that is assigned to that secretary in terms of directives and how individuals are appointed or how decisions are made. again, it goes back to my comment that it is me and my health care that we're talking about, i want to know that it is me and my doctor who are talking about it, or if i need have other family members in on the consoles, that that is where it is. quite honestly, i don't think that having a group of nameless, faceless individuals that are
6:28 pm

telling my doctor what he should be doing for my health care is where i want to be. [applause] >> the gentleman with the glasses, that road back. yes, sir. could you please introduce yourself? >> senator murkowski, my name is darryl. would you support a public option if it saved the overall economy in the long run? what i mean by that, $100 billion a year federal increase but it would save the economy. there is now a hidden tax on insured people, about $1,900 for each in chirred worker in alaska -- ensured -- insured worker and alaska.
6:29 pm

it rivals are in come taxes, $3,800 between the two of us. also, a 50% of bankruptcies, 62% of foreclosures -- those are costs to society and they are due to medical bills. if you took the long run and saw that the overall economy would help, which he did support a public option? -- would you i haven't asked many times -- i have been asked many times that i was just spoke -- a five would support a public option. i remind you bet it does not so much that a government-run plan is in and of itself a bad thing. we had a government run right -- government-run health care right now with medicare and medicaid and aid va system and be ihs system. we have that.
6:30 pm

i am not afraid to say that we cannot absolutely positively not have a government-run plan. but what we have to have is a government plan that actually works. and let me tell you -- [applause] to take the model of a broken system, a system that does not work, and in the system of met -- and in the state of alaska, medicare does not work. if you cannot get in to see a provider, it does not work. if we're going to move toward any kind of government-run plan, that that all is clearly going to be in the details. if you cannot get in to see a provider, all we are doing is giving new a new card, someone describing it as giving someone a bus ticket knowing full well
6:31 pm

that there is no bus. that is wrong. that is wrong. i am not just say no to a government plan. >> as go back to the gentleman in the brown shirt, about halfway back on the right. >> thank you, senator. >> please introduce years -- yourself. >> my name is ray and i am one of your center -- senior citizens. not your fellow senator nor are president nor many members of congress have something that you have, our credibility -- your credibility in our trust. -- and our trust. [applause] britney when i say that high and many of our fellow senior citizens are terrified at what can happen to us if this
6:32 pm

hurriedly and haphazardly written bill is jammed down our throats. i went down to my doctor yesterday. i got extra hour -- x-rays and an mri. it was so comforting to know that i was covered by medicare and i did not have to get to that government alpanel to telle whether i can have it or not. they know i can have it or wait like so many other countries. the bottom line, and my question to you is this, because i cannot believe the smoke and mirrors and the bait and switch signals coming from the white house. how can you add 40 million people to 50 million people to medicare, cut $500 billion from the program, without rationing and giving people like me and the elderly any of these other services that we're going to need? it sounds like they're going to
6:33 pm

be doing a lot of rationing, denying and deferring. medicare does need to be fixed, but much of it works right now. you had mentioned what needs to be fixed. why throw the baby out with the bath water? why we fix what is wrong -- why don't we fix what is wrong? [applause] >> i appreciate the comments and what you have expressed is what i have heard from so many. why for the baby out with the bath water? well, i will tell you -- and it goes back to my comments to the last gentleman. we have got a system here and alaska that is failing our seniors if you cannot get in to see a provider. you're going to hear me say that many times tonight.
6:34 pm

i have got to figure out a way where we can address the concerns and alaskans and people all of the country about the rising cost of health care, the rising cost of premiums, while at the same time providing new access to a doctor, somebody who can write your prescriptions and heal your body, fix you up, and our reality is right now we are not doing that. the legislation you have suggested has been rushed through. i will tell you. we have a process in the event -- a senate health committee -- in the senate help committee, it was not a good way to deal with the bill. we had at thousand page bill, presented to us for the first time on thursday night, and we were told that we would markup on tuesday morning, have your
6:35 pm

amendments in by the week ended and the section on the government option was not even included because it had not yet been written. we spent four weeks going through all aspects of the bill, but it was a process that in fairness was not a real effort to work through the tough issues in a bipartisan way to make a bill better. the pressure on us was to get the bill at committee yesterday. when you set an arbitrary date for the accomplishment of something, and you do not set as your priority adapting good policy, what you what it is something that moves out of committee that is not good policy. i am not willing to support anything that is not good policy.
6:36 pm

[applause] . i wish i had more details about it. i make contact with the senate finance committee just today to say, do you have any more in terms of where you are with the specifics of a co-op? the people of looking at this. is this a way for us to go? what i was told today is that in
6:37 pm

fact there was a great deal of discussion about the concept, that it may be something that can advance through this group of six after working and be presented to us. -- that are working and be presented to us. right now it is more of a concept. i wish i could share more with the. there are some who had said that we cannot go with a co op, that we need to stick with a public option there are. others said they cannot go with the co often because it is nothing more than a trojan horse for the public option plan. we are going to have a clashing in the meeting. right now we do not know what it is. here and alaska, we have familiarity with our rural electoral co-ops. how would that work within the health-care field? i do not know that we know yet. is this something that is worthy
6:38 pm

of discussion? why should we not talk about it? why should we not take the time to look at all of the options and all of the issues incident saying this is the path that we must take and we must take it by the state? let us put it out on the table. [applause] >> the woman with the blond hair, blue, about half way back. this way. this side. right in front of you. right there. with that lady. predicted that lady. >> i work for a medical billing office. my concern is that we will get into the same situation we have with medicare with the reimbursement late -- rate so low and people cannot stay in business with the amount they reimbursed. if we do go for something from the federal government, are they
6:39 pm

planning to cap fees and push doctors out of business and then we will lose all of our doctors? >> i wish that the gift is something comforting their credit -- i wish that i could give you something comforting there. the reality laid out by the director of the cbo is that in order for the health care plan that was moved to the health care committee, in order for that to cancel out, the reimbursement rates under a public auction would have to be set at medicare rates in order to work. at one point in time, we were talking about medicare plus tender. i met the group of doctors. i said, if we did have this plan and that was the reimbursement rate, what would it mean to you? to a number, the also, i could
6:40 pm

not do it. i could not do it. you not only -- you would have doctors who are not only opting out of medicare, but would opt out of the government plan. whether it is the senate bill or the house a bill that we are looking at, the house bill put it at medicare plus 5%. doctors in alaska are saying we simply cannot do it. again, we are trying to -- the structure that has been built in the senate health committee and house side is one that is built too similar to a system that is not working for a rural states like alaska and will not work for other rural states. it might be working just fine if you are in washington, d.c. are in boston or in a big urban center. it is not working for us.
6:41 pm

>> excuse me. this way. the woman right there. she has a gauge-ish ---- eight beigish -- >> i am here representing 16 family practice doctors, which is 20% of the family practice doctors in anchorage. we went from 180 down to 70 because of a medicare reimbursement rates. if the bill that is currently proposed, we would all be out of business by 2014. this is a very serious problem we all enjoy seeing our patients. right now for a $150 office visit, i am paid $14 by medicare. $40 by medicare. they made $3 billion lester. what we need to do is allow our
6:42 pm

seniors to take $300 that they are paying right now to the secondary insurance, put it in savings, so they can pay us, hearing aids, other medical devices without a bunch of government bureaucracy. people should be allowed to do help savings accounts but if that is one of the things we need to change. [unintelligible] several of my colleagues have dropped of the medicare. there are other different things i would like to see. one is business offices for patients that cannot afford the health savings account to allow us as physicians to write off these losses as business losses. none of these things will cost the federal government a penny. it would pit the control back in the hands of the patient and of
6:43 pm

the physician. we also need to reform malpractice. that is not addressed in any of these issues. [cheers] i have already been built -- >> thank you very much for your comments. you reached your two minutes. that was great. >> on this side. the gentlemen three rows back. >> before we go, what i want to do is acknowledge your and thank you as a family practice doctor. you are, unfortunately, almost a dying breed in our state. what is happening is the government is driving those out of practice. it is people like those in the
6:44 pm

room and those that are listening and watching that suffer the consequences. you offered some good suggestions. i thank you for them. >> now down to the front. third row back. you with the glasses. thank you. >> thank you. i am a small business owner here in anchorage. i provide health care for my employees. i they have a health -- they have a coke a. the most inefficient part of my company is dealing with the government. municipal, state, and federal. every part of the government that i deal with is inefficient down to the post office. [laughter] [cheers] why would we why would we want to allow the government to be in charge of health care in the united states
6:45 pm

when they cannot do anything right as it is? thank you. >> you run a small business and know what it is like to be in charge and make decisions for you and your employees and your family. i think that many of us recognize that when you lose control of bayh, whether your state government that takes control of your federal government even further away, the decisions may be more attenuated than what you are able to do. i do not believe that we in the federal government should be running health care. elieve that we should be building automobiles. [applause] the government is good that some things. do not ask me to tell you what they are right now. [laughter] that is a completely different issue. healthcare, and i think this is
6:46 pm

what has driven you out here today, is personal. it is often times emotional. for us at the government level to impose more than a one size fits all standard, i do not think you get the level of decision making that you want and the ability to choose that you want for you and your family. the direction that we are taking great now, i think we need to fall back, revisit how we can make meaningful changes that do not cost this country and provide better health care for all americans. >> i have another comment from the folks out side. this is one -- how will we prevent insurance companies from placing financial limitations or caps on how much they will pay if we have not been able to do that already? >how can we actually do that?
6:47 pm

>> i want to acknowledge the people that are in the back of the room. i do hope that most of the a able to sit. i see some standing. the good news for you is the air is probably a little bit settling on the outside. you may have had the better end of the deal. as far as how we reckon with and deal with the insurance companies, i will tell you. so many of the proposals that are out there, whether on the house side or on the senate side, and what the president is talking about, many of these issues that relate to health insurance reform our reforms of the insurance companies are willing to take on. we are talking about the requirements that the preceding conditions -- if you have lost a job and to have lost your
6:48 pm

insurance and you have to move to another insurance plan, you have a pre-existing condition. i think there is a recognition. this is something that shelby and will be addressed. -- shelby and will be addressed. -- shall be and will be addressed. that is one of the issues. there is another area i think we will see a bipartisan result on. it is because the demands from the american public is such that we -- why would you stick with your insurance? why would you continue with a program that you do not know if they are going to -- if they will say sorry, you have now covered a new love. we are no longer a going to be covering you. these are some of the reforms that, again, are areas where
6:49 pm

republicans and democrats are an agreement that we need to resolve. [applause] >> in the back of the room, i think it is a lady with a green shirt and hat. yes, thank you. >> thank you for having us tonight. i just wanted to give my 2 cents. i feel like this plan, the president, the house, the senate is a recent visit of socialism. -- rep of socialism. i am very afraid of that. i think they are trying to come in softly through the back door. i just wanted to say that this is not the country that i want to the then it goes to that bit of [applause] [cheers} >> your comment is one that i have heard expressed.
6:50 pm

it is not specific to this health care bill that we have in front of us. it is a concern about a draft that we may be seeing in the nation. i think it should concern us. >> over undecided the room in the back. the gentleman with the hat in the back. >> can you wait for the microphone? but it is the gentle man with the brown hat. thank you. >> hello. i may be beating a dead horse to death. i am hard of hearing and have not heard all the answers. i do have something to say about the medicare reimbursement rate. if you are not on medicare, for
6:51 pm

your information, if your doctor charges you a thousand dollars, medicare will probably reimburse him possibly $250 for the payment. this is one of the region's -- reasons doctors are not seeing older patients and medicare. i do not what predict i do not know what you will do about this, because the few increase the rate and the amount of spending that the government option will go up. if you go pass a law ordering them to see these patients, i have no idea what is going to happen. my other comment is that i kind of see this as we are driving along in our automobile and up the road there is a big fogbank. it is complicated by the medicare payment system, by the poor people not having enough coverage, by rich people being able to get whatever they want,
6:52 pm

and i feel like it is as though we do not know where we are going. it is going to take a lot of working together on both sides of the aisle from the republicans and democrats to find the solution to this problem. i have not seen a lot of positive things come out from the republican side other than some negative comments, we do not want that, we do not want this. i would like to see more working together. we need it. it is going to take something like this to solve it. [applause] >> i agree wholeheartedly with you. it'll take more working together. it is going to take more time. this icomplicated. this is complex. it is not going to happen because i say that we have to
6:53 pm

have it by this date. think about what we are doing. this is 1/6 of the nation's economy that we are talking about. we are talking about health care reform. this affects you with your democrat or republican, urban or rural or live in alaska or maine. this process is everything. let's take the time to get it right and if it takes us a few extra months, it takes a few extra months. you mentioned that we need to be working together. this cannot be just a democrat solution, because it is not a democrat problem. it is not a republican problem or a republican solution. we have got to figure out how we address this issue that affects all americans. we are very divided in the congress right now.
6:54 pm

in order to get to solutions that are workable, we have got to figure out how we come together to have a good discussion, a good debate, and work through these issues. there are a couple of good bills i think that are out there on the table that had been procured by republicans. there is a bill from oregon and utah that they have put on the table a year or so ago. that particular one has 13 co- sponsors on it, pretty much even in terms of a republican vs. democrat. there are things in it that i do not like, but is the meat of is something that we can be working off of and talking on it? yes. this is where we need to be going, not necessarily saying it
6:55 pm

has to be this bill or it has to be this plan. we have got to be sitting down and we have to be doing the hard work. there are six men and women in the finance committee that have said i am going to hold off all the pressure i am getting from republican leadership or democratic leadership or the president and they are saying that we have to plow through and work on this. will they do it? i do not know. i am sure hoping that they have the collective will between those six to continue it. i think americans want a solution. they do not want to see the partisans disagreeing and bickering and name-calling. they want to see solutions. that is our job, to deliver solutions that work for the country. i agree. >> the lady sitting at about 6 rows back with glasses. this way. thank you.
6:56 pm

>> thank you for being here. i have several questions. i am a 44-year-old disabled person. i am on social security disability. i am on medicare, they are for. as the gentleman stated in the back, medicare only pays between 2% and 20% of what the physicians bill. it is incredible. 1200 other bill and they will pay $47 or less. in some cases, and they pay nothing. that is the reason why our doctors are opting out of medicare. i do not blame them. as far as what you are saying you will support about health care reform, i would like to know who guarantees that i can even see a doctor? i would also like to know who
6:57 pm

and how will it be decided whether my life style is help althy and my behavior's arm healthy i will beeworded by that by continuing to get health care? as far as our small business employers, hawaii, which i lived in for 12 years, is the only state with mandatory employer coverage. if your job is 20 hours a week or more, your employer must provide you with healthcare. what that has done is hawaii is it has for small businesses to hire twice the number of people and have them work only 19 hours a week so that the small businesses do not have to pay for their health insurance. that is why most people in hawaii work three jobs. who is going to tell the employers how many hours a week a person has to work for them to
6:58 pm

pay for their health insurance? >> thank you for your comment. but that is a good comment. let me address the last one. in the senate health bill, there is a requirement that all employers who employ over 25 employees, they are required to have health care coverage offered to their employees. the year to do so will result in a $750 per employee penalty. if you are a seasonal worker or a part-time worker, the penalty per employee is $350. it goes back to -- he said u.s. small-business men. i do not know via more than 25 employees. one of the concerns that we have is if you have this
6:59 pm

employer mandate with the penalties on it, as a small business, you may but at what it costs you to provide for that level of coverage and say, you know what that's $750 as a penalty per employee, even though that is a top hit may be less than what i would be providing for coverage for them as is. i think i'm just going to stop offering my employer base plan and let them go to a government option. there is discussion about a government auction ultimately resulting in a shift of 80 million americans from private insurance to a public plan. you ask an excellent question about -- had to guaranteed to
7:00 pm

get health care. -- how to guarantee that to get health care. that is part of the problem. what is the guarantee? @@@@@ @ @ @ @ @ @ @ @ @ @ @ @ if you are an individual with disabilities and you had issues here -- say, you are on medicare. i should like you -- i should i use u.s. a specific example. how do people get health care? we might be able to guarantee a date -- guarantee that you have access to health care insurance. it does back to what was stated by the doctor earlier that if you do not have doctors that are seen this individuals, they are not taking medicare or on
7:01 pm

the government plan, we have given you the's ticket without the bus. said you nowteed access said you nowteed access have insurance, but if we . it, witches of getting you in the door to see a provider to help you, how have we helped you? again, to go back to building a system of reform on a system that has failed this year in alaska with medicare, it goes back to the reimbursement issue. it is just not going to work. we will not be able to guarantee you health care. we might deal to guarantee you the card that says you can get it. but if you are living in the wrong spot, [unintelligible] wrong spot, [unintelligible] >> this the thing compared to
7:02 pm

the size of the federal government. government. but i do not want to see the federal germond grow. i want to see a trend. i just went to technical school for major airline. we have people from my company from all over the world. i was sitting next to a guy from england. he had an emergency operation on a hernia. they put him on a six month waiting list. six month waiting list. he had to hobble onto a plane and fly to new york and got the operation the next. what are we even thinking?
7:03 pm

the government is not one to be able to do this. [applause] >> when i went to fairbanks for the town hall meeting last week, i talked to a man whose family lives in canada. he said, please, do not use this as a model. he said let me tell you about my uncle who had in issued with his knee. he said the made him wait for six months before -- excuse me, four years -- it was a long
7:04 pm

time. it obviously was not as pressing as this individual you address. they made him wait for four years. it was not because there were not the doctors or the providers to care for him. he said they wanted him to wait until he hit 60, because they estimate that a knee is a good for about 20 years and it did not want to have to do two knees. that is not the kind of health care that i want. >> down in the front. the gentlemen on the second row with glass. >> first of all, something we can all agree on is mortality is not 100%. other than that, why do not we tail of the profit and bonus vaulters to run this country's healthcare now and give them an average 3 year price for their stocks and a credit for their income taxes or their capital gains taxes, buy all their
7:05 pm

stocks, and make health care and health care delivery profitless, cooperative, and a mutually owned? i had usaaq insurance for my home and my car and i get returned on my premiums every year. i have an saa account which people in the u.s. they do not know about. the $400 that i can take with me. i could take with me. my premiums have gone up may be 1% in the past 20 years. i have the $400 in the bank. i get a return to my premium dollars every year. that is what we need in healthcare. i use to the physician, but i quit because of health reasons and because of medicare and insurance reimbursement procedures and road blocks. i could not take it anymore. i am sure there a lot of people who are out there who would not
7:06 pm

mind a nonprofit, patient oriented health care system funded by the premium dollars of the patient. i estimate that if you charge $4 a day for people who love nothing wrong with them, $6 for 50% of the people who of wonder to problems and $8 a day for people have 34 problems, you could raise $650 billion a year. >> your time is up. >> i will just pick up on your comments about a co-op in a non- profit entity. that is something that is out there in subject for discussion is a reasonable? absolutely. will it work? who knows. i think these of the types of things that we ought not be afraid to have out there on the
7:07 pm

table and give them due consideration. i'm sorry you left the practice. we need more of the. >> thank you. >> another question from the back. this is a number of the card questions. they want to know about tort reform and is the part of the discussion? [applause] in my opinion, tort reform has got to be part of the discussion in. it must be part of the discussion. you talk with the doctors out there. we have one that is a family practice. we will have one that left the practice. all those that i have had an opportunity to speak with admit that there is defensive medicine that is being practiced every single day in all parts of the country where you have a doctor's. it is because of the fear of
7:08 pm

being sued, the medical malpractice and the liability. the doctors know what it is he or she should be doing, but because of the threat -- ere is going to be extra careful and ordered just one more test to be sure. when in fact, these men and women and professional but have been trained, they know what they are doing, but the way our system works -- where the most litigious society in the world -- we put our providers in a box. we say, you should have done that or you should have done that it has. if they are ordering perhaps unnecessary tense that cost all of us. it must be part of the discussion. the estimates that are out there have turned from the cost to
7:09 pm

the health care system, put it in the range of $100 billion. we have to be realistic that when -- if we are going to meaningfully address the ever rising cost of health care, we have to look at tort reform as one of the issues. it is not part of the bill that we have coming out of the senate tried now. it is not part of the house package of the polka i think it is neat -- part of the package. i think it needs to be. >> three thirds of the way back. a woman in an orange shirt. >> you are pretty good at spotting them. >> why is it part of the
7:10 pm

discussion -- one thing i'm going to ed is this mentality they you do not have to abide by the laws you pass. if you pass something, you better have to abide by it. [cheers] >> i am with you on that. we should not have our own special program. right now as a federal employee, and member of the federal employees health benefit program. my program at the united states senator is exactly the same as the 17,000 other federal employees that are here in the state of alaska. here is the deal. if we were to pass a government run option, i believe that we as members of congress and those who work for us, should also be
7:11 pm

part of that plan. there is no reason that we should not. [applause] that is part of the bill. it came out of the health committee. it came out on a narrow vote, 12-11. it was interesting how partisan it was. it was interesting how partisan tort reform is. we cannot seem to get our democratic colleagues to come with us in agreeing that tort reform must be part of the equation. we have to work on that. >> the gentlemen in the yellow shirt over their standing up. >> everyone, please introduce yourself. >> thank you very much.
7:12 pm

i have been in the insurance business for 19 years. i have a stake in this discussion as a result -- discussion, and as a result, i want you to know that i am on here on behalf of my clients. there was a meeting that went on with the senator hollis back in january or february. he had a similar discussion. 90% of the room was people who were affiliated with the health insurance business, doctors, and nurses. i made this suggestion at that time to him. i think that reform is a huge part of this. the litigious society that we are has stepped up the pace for the cost of the health insurance to the people at large as a result of their increasing premiums. there is also the research and
7:13 pm

development that we paid for as a society that does not get passed back to us. it gets passed on to us at a cost item. if we were to take the research and development for the prescription medications that are necessary for everyone involved, especially our elderly now, that would be something to look at as far as a reform. we need to look at the manufacturers of the equipment that is used in the doctors' offices and make sure that that is positioned correctly on the cost basis of the doctors can afford to get it. the cost of the buildings that they have to build, the on and on, if you take it step by step, i think what we are doing is looking at a reform for health insurance, but we really need to look at the basic costs and drive those down. one thing that is really missing is taking our children and offering them an education --
7:14 pm

>> your time is up. >> the gentlemen at touched on an interesting point. i actually asked this this morning. what exactly are we talking about when we talking about health care reform? it is something that we need to better -- refine. are we referring health care insurance? that is one aspect of it. do we need to reform medicare so that it works in states like alaska? absolutely. do we need to the reforming the delivery system and how for instance -- how procedures are
7:15 pm

reimbursed. i mentioned at the outset that we need to be working toward @@@@@@@ we need to be looking to medical home models where you have, basically, a service coordinator. we have to be looking to how we deliver our health care costs and, thus, reduce those costs. these are all very different pockets. health care insurance reform is perhaps different than what we need to do with medicare reform and is perhaps different than what we need to do with reform and restructuring of the delivery systems here. again, this is very complicated. -- mike oginski who is the ranking member on the senate
7:16 pm

health committee has said -- every title of his health care bill that we have gone through could be its own stand-alone legislation. it is that detailed. it is that complex. ladies and gentlemen, we need to get it right. we owe it to you to get it right. [applause] >> over on this side. the gentle man with the light blue shirt. thank you. >> my name is john. thank you for being with us today. i appreciate that. it seems to me that basically it is a foregone conclusion that there is going to be some kind of bill eventually passed. -- past regarding health care. it seems that the democrats already have the numbered to pass the bill without any republican support. my question is, if we have a
7:17 pm

medicare system that currently allows doctors to withdraw, to not be a part of it, will the doctors still have that sort of an option we have a federal government mandated health care system, and if they are allowed to withdraw, and we have the same thing happen with this new system as we have had happened with the medicare, what is going to happen? >> that is my question. [applause] >> in the very back. a gentle man with a longer hair and glasses. in the middle. >> i hope he did not take that as a flip response. it is not. it is a very legitimate question. we do not have the answer. the fact of the matter is, those providers with opt out.
7:18 pm

>> ibm and uninsured americans. i know you are aware that we already provided nationalized and the single payer -- [unintelligible] it is in the firm of the ihs, the indian health service. they are usually critical of this. it gives the ihs good reading, reading moderately are fully effective. the only place with the ihs still isn't tradition of services to native americans to leave tribal lands or reservations to find employment or education elsewhere. it can only be fixed by nationally covering plant. firstly, if we as americans feel that the ihs service is good enough for people to whom we owe so much, people to whom we are
7:19 pm

making up for crimes that were committed a been spent, why is it not good enough for the rest of americans to have government help services? [cheers] secondly, if we feel that it is necessary that it is a moral duty to provide this help service to these people as the restitution for the crimes committed against them, why should we not feel as incumbent upon us to provide them to african americans or other form of the oppressed person kiddie groups who do not receive it? how is not a form of institutionalized racism? >> let us talk about theihs, because we do have here an increase particularly -- in
7:20 pm

anchorage reticulate, it is a first-rate facility. i think that we are proud of what they have been able to do. i have been on the indian affairs committee since i got to the senate. i have had an opportunity to really spend some time understanding being i systemhs, how it is working and how it is not working. we chronically underfunded ihs which has led -- you want to talk about rationing care, you go and talk to some of those who live on reservations in the lower 48. it pretty much if you have -- if you have injured yourself after july, you are out of luck, because the money in is out in terms of what is available to be paid. it is a pretty dismal situation. i think we look at ihs and say that there are -- that it is a system that when allowed to work
7:21 pm

with the appropriate financial backing and support, it is ok. it is not a model of government efficiency. i will speak to another form government health care we know about in this state, that is the v.a > i can tell ian that if you happen to be -- i can tell you if you happen to be a veteran who happens to live in an area where you have access to v.a. services, that is good for you. far too many of our alaskan veterans, whether they live -- they are basically is no access. they are given the promise that they earned when they signed up to serve, that of health care, but only if they happen to live in the right place. is that what we want to be doing? i had an e-mail from a woman who
7:22 pm

said, i am on medicare, my husband is a bet. i cannot get him to see a doctor and my husband has been waiting for three months for the be 8 to sign off on a prescription drug that his doctor has ordered that he take, but the v.a. cannot decide whether or not this is something they will be paying for. we have some issues with a government run systems. again, if you are going to go down that road, you better figure out how you do it right, whether it is standing by the obligation to american indians and alaskan natives. >> the person in the middle with the green shirt. >> is nancy here?
7:23 pm

>> no. >> my point of talking is that i had something done to me directly i had my cataracts removed. they said i needed the skin from the inside of my eyes removed because i had no side. they gave me list some doctors. i took the first one. i went over there. i saw him. he said that he could fix it. they pulled of the muscles from my eyes and removed the skin on the side and pulled them up. i went in for the operation, was unconscious while he was operating. he did 21 things wrong to me. i tried to get to the insurance to not pay him. they paid him. then i went to its 34 attorneys and they will not go against the doctor.
7:24 pm

even out a separate did i went to lower 48 to get some doctors to pass judgment on the operation. they called the doctor up here and said, they could not help me. what we have here in alaska is that the insurance companies, the medical malpractice -- there is no help for people who have medical malpractice. as far as the v.a. is concerned, i have a printer is in the air force. he was held prisoner overseas. she was being treated for posttraumatic stress disorder. the v.a. here was treating her. then they stopped and said that she had to pay full payment because it was her choice. >> on the issue of tort reform. there are many who have concern that if we were to institute a
7:25 pm

level of tort reform that the doctors did act negligently that they escaped free. that is not what the tort reform is about. it is not designed to let doctors fail in their practice. again, it is making sure that the protection is there for the patient. -- patient, while ensuring that at the same time we do not have a practice of defensive medicine that unnecessarily costs people across this country. >> of the gentlemen in the red shirt on the front row. >> my name is ed. i was wondering, how come -- senate and house cannot get their act together into maybe
7:26 pm

put a levy or higher tax pay for our medicine from the imports we are getting in from communist countries? why do not we give america back to america? [cheers] >> i tell you. i am not one that what my health care shipped overseas. i am not one that once we did i want to make sure the drugs that i am taking part are safe. they are the drugs that my doctor has believe he has prescribed for me and the medication that denny. you are talking about a bigger picture, which is keeping the local and bringing it home and supporting americans. that is a tough one to argue. >> back out to the -- there are a number of questions having to do with the providers with the
7:27 pm

shortage of physicians of practitioners and other providers. is there anything in the proposals that discusses that? >> in both the senate bill and the house a bill, there is a recognition that we do have a shortage of providers, particularly in the primary care area. some of the proposals that are out there are ways that we can in sent individuals to go into practice, whether it is payment of student loans so that they can be encouraged to come back. we need to do more to get more providers. it is not just here. there are 17 states across the country where right now there are simply not enough providers available to accept specifically those on medicare. it is states oregon, washington,
7:28 pm

colorado, new mexico -- this is an issue that must be addressed with how we deal. it hurts us more markedly in rural places and in a state like alaska where we do not have our own medical school. we are not growing our own. one of the things that we know is that typically an individual will and a practicing within about 100 mile radius of where they have been training and established their residency. we are kind of out of luck in terms of that. we are working with the university of washington. we are working with providence -- they have a training program. our reality is that we are at a disadvantage. we do have things in the legislation that does focus some incentives to encourage
7:29 pm

more to go into the practice. one of the things that i think we need to do is recognize that it does not have to be just and senses to be a doctor. we need to have more mid-levels. we need to have the nurse practitioners. we need to have the p.a's. we know that so many communities you will never have a doctor out here. let's make sure that when be talking about reimbursement that those mid-levels are covered as well. we need to do much more to encourage those to go into the primary care as opposed to the specialists. right now the incentives are not there. when you talk to a cardiologists about what they get reimbursed for a procedure purses a family for a procedure purses a family care doctor is going to get
7:30 pm

we need to turn that on its head as well. there's a lot that we can do to provide the appropriate incentives so that we get more practitioners. >> the lady in the back. on your left with the blue shirt. >> greetings, senator murkowski. i would like to make an observation. it seems that, as soon as the american public becomes familiar with what the definitions of like health care, insurance reform stands for, you guys morph and change it to a different name, such as health insurance. which is it? is it health care? or isn't health care insurance -- or is it health care
7:31 pm

insurance? or is it health care insurance reform? or is it a co-op? which is it? >> that is the process. it is. it is difficult to follow. we are all smiling and laughing, but she is right on. right now i think what you need to understand is this is still in process, a legislative process. and they describe it as sausage making. that is probably an acpt description for the you do not know what goes into, but you want to know that the allen goes good. is it a government option, is it co-op? that is why i am out here listening to you and getting your input. >> over on this side. stand up.
7:32 pm

>> we are making these guys get their exercise. so much for the prevention and wellness. it is not working. click the button? >> palin? thank you for coming. thank you for having the courage to come here and in person rather than by teleconference? i have a couple of comments to make about what the definition i believe of health care should be. i hear a lot about money and profits and want to remind you we are talking about lives, health, our grandparents, family members, and our communities. profit and money is one thing. we are talking about human
7:33 pm

beings. the second thing is along the lines, i think that profits and health care are morally -- a morally should not be connected. period. they are not together. you cannot have profits associated with making the right decision of the time. when you have a profit in there, you'll never make the right decision. maybe sometimes, but not always. i want to ask you how you like your healthcare. >> i am fortunate. i have health care. i am fortunate. i have health care. it is the same health care that other federal employees around the state capital of the thing that is great about my health care. -- i had a couple of dozen
7:34 pm

plants as i can choose from. by more than a couple of dozen. i have p a i havelans that i can choose from. -- i have a lot of plans that i can choose from. i think this is what people want. when my kids were younger, i wanted to make sure that we had something in the plan that was either able to put aside something in n saa or you are dealing with the means that we planned for as a family. when my husband and i first got married, we were not making a lot of money between the two of us. we wanted to make sure we had coverage provided maternity benefits. you just figure it out. you spend money on your healthcare then you want. the point that i am making here is that i have, as a federal employee, i got choices within a
7:35 pm

suite of options that is offered to me. i think that is what people want with bill healthcare. they want choice and they want to be able to streamline it to their needs and to their families need. as you change and grow and family grows, you change your plan. you want to have portability. how many people do you know that are stuck in a job that they do not like that they do not dare leave because of the health insurance? they are stuck there. that is wrong. when we talk about those things that we must fix -- that is one that we must fix. >> over on this side with the blue shirt next to the lady with the red shirt. there. but do you feel like you have won the lottery when he calls on you? >> i would like to see before
7:36 pm

showing up today. i appreciate that a great deal. i think it is also a neat thing that we as alaskans can come together. we are not like the other states yelling and screaming. [applause] i -- i am a former marine. i like to be pretty keep things simple. my problem is that we have been told that our system is completely broken and destroyed and had to fix it right now. 88% of americans are satisfied with their health care plan. does it make sense that you can add that large of a number that have access to it, have it, and by these numbers are happy with it are satisfied?
7:37 pm

doesn't it seem more logical and easy to manage if we do with those that do not and to try to take such a large step and say you cannot have what you have worked for? . . i have worked to attain what my family needs. we cannot continue to try to work both sides of the offense, pulling on both ends, and having a middle-class that is torn by two sides. if we can deal with that percentage that is not happy and cannot get it or is struggling to get it and leave us to have what we -- to have what we have, i don't understand how you can see say that it is completely
7:38 pm

destroyed and we need to change it right now. [applause] >> first of all, i think you for your service. secondly, i think you for articulating what so much of our problem is. if you look to the chart that i provided you, in terms of the breakdown of the 47 million uninsured, we have been talking collectively as a congress and saying that this is the group we need to address. we need to provide them insurance. again, i will take you around that part chart. when you get to it is 12 million or 13 million that are really those without affordable insurance options. they just do not have anywhere else to go. they cannot. they not eligible for s chip or medicaid. and they are legal citizens here in this country and they do not have the income that would allow
7:39 pm

them to do this. we are talking about about 12 million. 12 million is still a lot of people that we need to address. [applause] but it is not something that, again, in order to address that need you throw out everything else that is working for 177 million people [applause] -- 177 million people. [applause] so here is the challenge. that is not my statement about whether or not any 9% of americans have health coverage and 88% are satisfied with their health coverage. we took a "time magazine" pau p. there is great concern that when
7:40 pm

you're talking about health care reform and you do not have -- and you have those with valid option for affordable health care coverage. but you and your family have been working hard and a satisfied with where you are. the concern is why are you missing with what i have? this is a great tension that we are seeing around here, trying to figure out how we address those who are truly without without messing it up for those who like where they are and would like to continue with their current coverage. it is a very difficult issue. [applause] >> about 10 rows back, there is the young man with the blue shirt. >> thank you for coming today,
7:41 pm

senator macau kit -- senator murkowski. . senator reid and the majority whip recently said that they would not be opposed to passing health care reform if they do not have the necessary votes to bypass a filibuster, that they -- i do not understand budget reconciliation. i was wondering what you think about that and whether that is a feasible solution. for the record, i do not think that is a good idea. [applause] >> the budget -- the process of a budget reconciliation is a system that is unique to the senate that would allow for a way to get around a filibuster it requires 60 votes to break it. when it moves through reconciliation, it only needs 51 votes. it is a process that is available.
7:42 pm

it is a process, however, that is subject to some technical rules within the senate in terms of what may be considered under reconciliation. without getting too much into the wheat, there is so much contained within the health-care bill that came out of the health committee that would not be subject to reconciliation. for example, the wellness prevention pieces. what would be subject to reconciliation would be the tax peace. here's the question to you. if you're a democrat and you are saying that we have to move this plan because our leadership has directed that we should, if all you're going to be able to move is the tax peaiece without considering the good things that are in the bill -- i think that
7:43 pm

the wellness and prevention pieces are good and necessary -- is that where you're going to be as a member representing your constituency? the republicans do not like that. a continue that for effect. we need to be working together on a bipartisan bill and moving a bill that can get 70 votes or 80 members to support it. but it is an option for the democrats. they are in the majority. they have a sizable majority. they have 60. they have some options that are available to them. but i do not know. i am not in these other states during the august break. i am in alaska. i am listening to what alaskans are telling me. if i were a representative from some of these other states where people are coming out in droves and are expressing their concern about this, is wanting to go ahead and follow your leader.
7:44 pm

it is another thing to be listening carefully to your constituents. i think there is a dilemma out there. [applause] >> about in the same position on this side, the lady in the black and blue. [laughter] [laughter] no, that one the people were not as concerned with the huge amount of money we were spending -- at 4. >> slow down just a little. >> with health care coming -- when we went to war abroad, people were not as concerned with the huge amount of money we were spending at war, hurting people. but now with the health reform bill that will help people, money is a huge issue. [applause]
7:45 pm

as the youth that will have to pay off all this money, i would rather use it to help people rather than killing them. [applause] everyone keeps saying that americans are creating a huge debt that their kids will have to pay off then why not ask us? [applause] >> i appreciate you being here. i appreciate your comments. would is happening of federal spending, whether it is on the men and women that are serving us in iraq and afghanistan, whether it is on health care, or whether it is on cash for clunkers, the fact is that that debt is sent to you.
7:46 pm

the choices that we make and the issues that we advance her, and lead darn well better make sure that we're doing it right and we are doing right by all americans. i wish we had more people like you are willing to stand up. ng to stand up. [applause] >> the woman appeared, the red shirt, about the seventh row back. -- the woman up here, the red shirt, about the seventh row back. >> my speech has kind of change to. you have been very good to us all. but we are scared. we are scared of what this administration is doing to us. they are taking away a good republican and replacing it with a socialist and we are scared to death. [applause] stand firm against cap and
7:47 pm

trade. the unions have too much control over this government already. [applause] through our apathy, some say that we deserve a are government and they might be right. but no more. the silent majority is speaking of with a roar. and we are not going to call down. we will not calmem down when you go back to d.c. we are mad. i appreciate everything you have talked to us about tonight, but i have so many concerns. there is the green movement, we're spending $10 billion in brazil for them to drill and they will not even let us drill in our own country. we are really mad. [applause] >> excuse me, we do need to stick to health care issues. [applause] >> you work for us. you have to fight for us.
7:48 pm

tort reform is the first thing we need right now. that will be the best thing toward health care than anything you can come up with. and we need to stop illegal immigration. [applause] that will help health care, too. [applause] >> she had on too many issues and i am supposed to stick to health care. i agree with you on tort reform. that must be part of our solution as we deal with health care reform. >> the woman in the dark black that is standing there. yes. >> thank you for taking my question and welcome back home senator mikulski. -- senator murkowski. i would like to thank the young woman from dimond high, bill linkx.
7:49 pm

i have two questions. do you have any ideas of what senator [unintelligible] ideas are on this issue? i am just asking. i am a registered nurse. i just got back from a seminar today it and i am finding out what medicare does and does not pay for and some of the things that i do as far as care for my patients. i understand there is all the stuff about insurance and who pays for this and who does that and the whole business. but my argument has and always been, for me, that patients come first. as far as the whole business on health care is concerned, i have
7:50 pm

only one question. how long is it going to take you to figure out how long is when to take you to do this? no, i am serious. [applause] we have had president clinton who tried to introduce it. his wife got into a little something. we had the bush camp in appeare. it has been 16 years? -- we had bush, come in. it has been 16 years? i did want to know what we are going to do -- i just want to know what we're going to do. >> thank you. [applause] >> i am not going to give you an arbitrary date and tell you that we must have it by this date. what we have to do is set as a
7:51 pm

priority -- we have got to get the best policy. if that means that we focus on insurance reform first and then delivery systems and then medicare -- i am not quite sure that we need to say that this one has to go first, chronologically, all wor we have to do them all together. it concerns me that we say it has to be done by this date. we had a conversation veered four of us were invited to the white house to talk to the -- we had a conversation. four of us were invited to the white house to talk to the president. i told him that signing on to an arbitrary date is difficult. he reminded me that congress is like kids in school and that we respond better with a deadline.
7:52 pm

and he is right there. but you set an arbitrary date and you push it and you get something that does not work for this country. we live with that for a long time did here is one thing that somebody asked me this morning. -- we lived with that for a long time. here's one thing that somebody asked me this morning. they said, is just money. it is not just money. health care reform is very important. the last time we did a really significant reform like this was back in 1965 and we have been living with that ever since. we need to make sure that we get it right. you have to ask my colleague for his specifics. [applause] >> up here, the gentleman in the middle, about the fifth row back. the white shirt. >> i guess i should thank you for being here mr. rakowski.
7:53 pm

my name is paul. i am not -- thank you for being here ms. mukowski. i am not scared. i want my old america back. i want my family back. [applause] and i want to be a free american dre. the problem is you and the other leaders. i have never seen such a disconnected leadership in my entire life. >> this is about health care reform. please ask a question. >> yes it is. because you are limiting 82 minutes, i have to make a broader statement. -- because you're limiting me to 2 minutes, i have to make a broader statement. will you asked baggage and young to join you on a three-day on
7:54 pm

camera agenda where we can ask probing an interrogative questions, you are not standing before us for accountability. as long as we have the lack of accountability we are going nowhere. [applause] thank you for allowing me to make this, and picks -- thank you for allowing me to make this comment. >> we had 690 people seated in this auditorium. i do not know how many people we had in the overflow. this is my small attend in anchorage to reach out to hear from my constituents. i did the same in fairbanks. we had about 600 people there. we're going to be in the peninsula next weekend. we're going to be in the valley on the following friday. we have to have a level of
7:55 pm

communication with their constituents. we failed to do that. we get disconnected. and we get pumped out. that is the way it works. you need to hold us accountable. i am not afraid of accountability. i am, i should not be in this job. let me stand before you and take the hard questions. i think we need to have this level of discussion and debate. i need to hear the ones that are angry and the ones that are just really sad andened. this helps me as i can best formulate on how i can best represent you in washington. you do not need to apologize for calling this out. have at it. >> ok, the lady in the front with the pink. [applause] >> thank you, senator. i am glad you're here and
7:56 pm

welcome home. i am a supporter of health insurance reform. and i seek your support in voting for the bill. if there is no bill, there is no reform. one of the things that i am concerned about is that, if you lose your job, you lose your health insurance. he few keep your job and do get sick, you could run into a cap and not have insurance in place. if you keep your job and go for preventive care, that is not covered by some health insurance companies. and if you actually get really sick, cumin not be able to be covered at all because it costs too much money. these are issues that must be addressed. it is my opinion that it must be addressed this year. the lady th said we have been waiting for 16 years for some kind of reform is correct. the insurance companies right now must be held accountable for the changes in public policy for providing additional health care
7:57 pm

coverage for all americans, not just the uninsured. [applause] >> you have articulated some money of the issues -- so many of the issues that alaskans are concerned about as far as health care. as far as doing something now, i do not need to tell you. i think you know that congress has a short attention span. again, i should not be flip. but our reality is that this is the moment. this is what we are working on right now. last year, which was a rebuff the focused on? energy. what was happening with the hype -- last year, what was everyone focused on? energy. what was happening with energy? health care is now front and
7:58 pm

center. i believe that we must be working toward some kind of reform. again, the devil is in the details. i have already had one opportunity to vote again the senate health bill. i do not think that it would help alaska or the country. i cannot go down that road. but i am not one of those that we just need to will this away. if we just wait it out, it will go away and we will not have to deal with it. it is not going to go away. i will take you back again to the graph that you have all been presented with. that national and federal health-care curve is only going to keep going up. the medicare kirk, in terms of where it goes, is just one to keep -- the medicare curve, in terms of where it goes, it is just going to keep going down.
7:59 pm

america is not going to forget about this. the woman in the back made a very important point. it was two administrations ago, with the clinton administration, the last time that we really tackled it. we did not pick it up for many years. i would be afraid of that scenario, if we were to put five years beyond -- between where we are now and do nothing at all and then wait about a couple more administrations. i am one that believes that we have a really tough job to do. but that is why you elected us to do it. it is not easy. we're not going to make everybody happy. but we cannot just say, if we wait this out, the american public is going to lose interest in it. our
63 Views
IN COLLECTIONS
CSPAN Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
